Aficamten: Discovery and Phase 3 Insights vs. Mavacamten in Hypertrophic Cardiomyopathy
From discovery to clinical development, aficamten outperforms mavacamten in PK, safety, and therapeutic margin. SEQUOIA-HCM, MAPLE-HCM, and ongoing ACACIA-HCM highlight its potential in obstructive and non-obstructive HCM.
Hypertrophic cardiomyopathy (HCM) is a common inherited cardiac disorder (1 in 500 individuals), often leading to obstructive HCM (oHCM) in two-thirds of patients. This causes left ventricular outflow tract (LVOT) obstruction, reduced stroke volume, and symptoms like dyspnea and fatigue [1]. Traditional therapies, such as beta-blockers or septal myectomy, provide symptomatic relief but do not address sarcomere hypercontractility driven by genetic mutations [1].
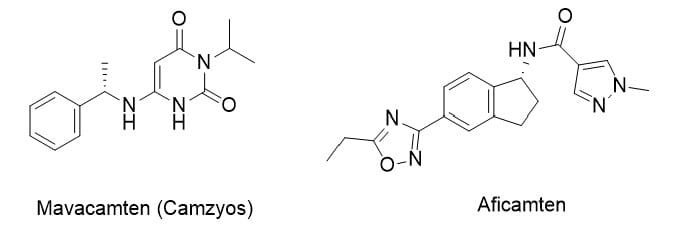
Cardiac myosin inhibitors (CMIs) offer a mechanistic approach by modulating sarcomere function. This post reviews aficamten (CK-274) from Cytokinetics compared to mavacamten (Camzyos, Bristol Myers Squibb) covering discovery, preclinical and clinical data, competitive landscape, the latest Phase 3 development in oHCM and non-obstructive HCM (nHCM), including the ACACIA-HCM trial, and regulatory outlook.
Discovery & Optimization
Aficamten was identified via high-throughput screening of bovine cardiac myofibrils, starting with indoline compound 1 (IC50 2.7 μM) [1]. SAR optimization of the indoline core, and later the 2,3-dihydro-1H-inden-1-amine (indane 12) core, improved potency 20-fold (IC50 1.0 μM) via hydrogen bonding to Leu267 [1]. Further modifications reduced lipophilicity and improved microsomal stability; the R-enantiomer was prioritized. Final SAR on the oxadiazole substituent yielded aficamten (ethyl variant) with balanced potency (IC50 1.4 μM), low clearance, and solubility [1].
Key Data Comparison
|
Assay |
Aficamten |
Mavacamten |
|
Cardiac myofibril IC50 (μM) |
1.26 |
0.6 |
|
Rat FS IC10 (μM) |
0.8 |
0.6 |
|
Rat FS IC50/IC10 |
9.9 |
2.8 |
|
Human t1/2 (actual, days) |
3.4 |
7–9 |
|
CYP induction EC50 (μM) |
No induction up to 25 |
2.2 ± 0.4 (3A4), 5.1 ± 0.2 (2B6) |
|
CYP450 inhibition IC50 |
>100 |
>30 |
Aficamten achieves shorter half-life, wider therapeutic window, and no significant CYP induction/inhibition [1, 2].
Preclinical Profile
- Mechanism: Binds allosteric cardiac myosin site, slows phosphate release, stabilizes weak actin-binding state → reduced contractility without affecting ATP hydrolysis
- Selectivity: Cardiac IC50 1.26 μM; smooth muscle >40 μM
- PK/PD: Bioavailability 41–98%, human t1/2 3.4 days, supports once-daily dosing
- Therapeutic window: IC50/IC10 ratio 9.9–13× vs. mavacamten 2.8×
- In vivo efficacy: Reduces contractility in feline HCM models; no off-target effects observed
Clinical Data
Phase 1
- Healthy adults (NCT03767855): Dose-linear PK, half-life 75–85 hours, steady-state in 10–12 days, minimal food/CYP2D6 effects. LVEF reduction max -5.5%, no serious adverse events [2].
Phase 2
- REDWOOD-HCM (NCT04219826):
- oHCM: LVOT gradient reduction -40/-53 mmHg, NYHA improvement 43–64%, NT-proBNP decreased
- nHCM (Cohort 4): 55% NYHA improvement, NT-proBNP -56%, LVEF -5.4% [3,5]
Phase 3
- SEQUOIA-HCM (NCT05186818): oHCM, 282 patients
- pVO2 +1.7 mL/kg/min (p<0.001)
- KCCQ-CSS +7 points, NYHA improvement 82%, LVOT gradient reduced
- LVEF <50% in 3.5% (reversible) [3]
- MAPLE-HCM (NCT05767346): oHCM vs. metoprolol, 175 patients
- pVO2 +1.1 mL/kg/min vs. -1.2 mL/kg/min (metoprolol)
- NYHA improvement 51.1% vs. 26.4%
- KCCQ-CSS +15.8 vs. 8.7 points
- LVEF <50% 3.5–4%, reversible [6,14]
- ACACIA-HCM (NCT06081894, ongoing pivotal nHCM trial)
- Evaluating aficamten in symptomatic nHCM (30,000–40,000 patients)
- Primary endpoints: NYHA functional improvement, LV mass reduction, NT-proBNP reduction
- Completion expected June 2026, potentially establishing aficamten as the first approved nHCM therapy [15]
Long-Term
- FOREST-HCM: oHCM and nHCM patients (36–48 weeks) maintained LVOT reductions, NYHA improvements, and LV remodeling. Safety: 4.3% transient LVEF <50% [3,5].
Comparison with Mavacamten
|
Feature |
Aficamten |
Mavacamten |
|
Human t1/2 |
3.4 days |
7–9 days |
|
IC50/IC10 |
9.9× |
2.8× |
|
CYP450 DDIs |
Minimal |
CYP3A4/2B6 induction |
|
Steady-state |
10–12 days |
~6 weeks |
|
NYHA oHCM |
82% (SEQUOIA) |
65% (EXPLORER-HCM) |
|
nHCM potential |
REDWOOD-Cohort 4 + ACACIA |
ODYSSEY-HCM failed primary endpoint |
Aficamten demonstrates faster dose titration, wider therapeutic window, and safer PK profile, with head-to-head or comparative advantages in oHCM and promising nHCM potential [1,3,5,14].
Competitive Landscape
- HCM market: $316M (2024) → $368M by 2035 (CAGR 1.36–7.8%) [3]
- Mavacamten dominates oHCM but limited by long half-life, narrow window, and DDIs
- HRS-1893 (Hengrui Pharma, out-licensed to Braveheart Bio): First China-originated myosin inhibitor to enter global race. ESC 2025 Phase 1 MAD trial: Favorable safety, PK/PD, rapid LVOT-G reduction (~90%) sustained through treatment [20]. Strategic out-licensing signals China’s entrance into the global CMI space.
- Other CMIs (CK-586, TN-201, ninerafaxstat) remain early-phase with delivery or scalability challenges [18,19].
- ACACIA-HCM positions aficamten to capture first-mover advantage in nHCM post-mavacamten ODYSSEY failure [5,15]
Outlook
- NDA review for oHCM in the U.S. with PDUFA date December 26, 2025, extended due to REMS plan submission [16]
- EMA and NMPA also reviewing aficamten under priority programs
- Potential Q1 2026 launch in oHCM, with ACACIA-HCM pivotal results to define nHCM indication
- Pediatric studies (CEDAR-HCM) and global regulatory pursuits ongoing [3]
Sources
- Chuang, C.; Collibee, S.; Ashcraft, L.; Wang, W.; Vander Wal, M.; Wang, X.; Hwee, D. T.; Wu, Y.; Wang, J.; Chin, E. R.; et al. Discovery of Aficamten (CK-274), a Next-Generation Cardiac Myosin Inhibitor for the Treatment of Hypertrophic Cardiomyopathy. J. Med. Chem. 2021, 64, 14142–14152, DOI: 10.1021/acs.jmedchem.1c01290.
- Robertson, L. A.; Armas, D. R.; Robbie, E.; Osmukhina, A.; Li, H.; Malik, F. I.; Solomon, S. D. A First-in-Human Study of the Selective Cardiac Myosin Inhibitor, CK-3773274. JACC: Heart Failure 2025, 13, 346–357, DOI: 10.1016/j.jchf.2024.09.012.
- Maron, M. S.; Masri, A.; Nassif, M. E.; Barriales-Villa, R.; Arad, M.; Cardim, N.; Choudhury, L.; Claggett, B.; Coats, C. J.; Düngen, H.-D.; et al. Aficamten for Symptomatic Obstructive Hypertrophic Cardiomyopathy. N. Engl. J. Med. 2024, 390, 1849–1861, DOI: 10.1056/NEJMoa2401422.
- Hartman, J. J.; Hwee, D. T.; Chuang, C.; Wang, J.; Wu, Y.; Schaletzky, J.; Sarkar, S.; Madhvani, R.; Edell, S.; Paliwal, P.; et al. Aficamten is a Small-Molecule Cardiac Myosin Inhibitor Designed to Treat Hypertrophic Cardiomyopathy. Nat. Cardiovasc. Res. 2024, 3, 1003–1016, DOI: 10.1038/s44161-024-00507-8.
- Masri, A.; Sherrid, M. V.; Abraham, T. P.; Choudhury, L.; Garcia-Pavia, P.; Kramer, C. M.; Barriales-Villa, R.; Owens, A. T.; Rader, F.; Nagueh, S. F.; et al. Efficacy and Safety of Aficamten in Symptomatic Nonobstructive Hypertrophic Cardiomyopathy: Results From the REDWOOD-HCM Trial, Cohort 4. J. Am. Coll. Cardiol. 2024, 84, 1789–1802, DOI: 10.1016/j.jacc.2024.08.020.
- Saberi, S.; Abraham, T. P.; Choudhury, L.; Barriales-Villa, R.; Elliott, P. M.; Nassif, M. E.; Oreziak, A.; Owens, A. T.; Tower-Rader, A.; Rader, F.; et al. Aficamten Treatment for Symptomatic Obstructive Hypertrophic Cardiomyopathy. JACC: Heart Failure 2025, 13, 102496, DOI: 10.1016/j.jchf.2024.09.013.
- Grillo, M. P.; Sukhun, R.; Bashir, M.; Ashcraft, L.; Morgan, B. P. Pharmacokinetics, Mass Balance, Tissue Distribution, Metabolism, and Excretion of [14C]Aficamten Following Single Oral Dose Administration to Rats. Xenobiotica 2024, 54, 670–685, DOI: 10.1080/00498254.2024.2397849.
- Sharpe, A. N.; Oldach, M. S.; Rivas, V. N.; Kaplan, J. L.; Walker, A. L.; Kovacs, S. L.; Hwee, D. T.; Cremin, P.; Morgan, B. P.; Harris, S. P.; et al. Effects of Aficamten on Cardiac Contractility in a Feline Translational Model of Hypertrophic Cardiomyopathy. Sci. Rep. 2023, 13, 32, DOI: 10.1038/s41598-022-26688-7.
- Saberi, S.; Day, S. M.; Masri, A.; Owens, A. T.; Olivotto, I.; Ho, C. Y.; Heitner, S. B.; Jacoby, D.; Sehnert, A. J.; Sherrid, M. V. Mavacamten: A First-in-Class Oral Modulator of Cardiac Myosin for the Treatment of Symptomatic Obstructive Hypertrophic Cardiomyopathy. Cardiovasc. Drugs Ther. 2023, 37, 211–230, DOI: 10.1007/s10557-022-07400-3.
- Heitner, S. B.; Jacoby, D.; Lester, S. J.; Owens, A.; Wang, A.; Zhang, D.; Lambing, J.; Lee, J.; Semigran, M.; Sehnert, A. Mavacamten Treatment for Obstructive Hypertrophic Cardiomyopathy: A Clinical Trial. Ann. Intern. Med. 2019, 170, 741–748, DOI: 10.7326/M18-3016.
- Grillo, M. P.; Erve, J. C. L.; Dick, R.; Driscoll, J. P.; Haste, N.; Markova, S.; Brun, P.; Carlson, T. J.; Evanchik, M. In vitro and in vivo pharmacokinetic characterization of mavacamten, a first-in-class small molecule allosteric modulator of beta cardiac myosin. Xenobiotica 2019, 49, 718–733, DOI: 10.1080/00498254.2018.1495856.
- Heitner, S. B.; Jacoby, D.; Lester, S. J.; Owens, A.; Wang, A.; Zhang, D.; Lambing, J.; Lee, J.; Semigran, M.; Sehnert, A. Mavacamten treatment for obstructive hypertrophic cardiomyopathy: A clinical trial. Ann. Intern. Med. 2019, 170, 741–748, DOI: 10.7326/M18-3016.
- MyoKardia, Inc. Form S-1 Registration Statement. US SEC filing, September 28, 2015.
- Garcia-Pavia, P.; Maron, M. S.; Masri, A.; Merkely, B.; Nassif, M. E.; Peña-Peña, M. L.; Barriales-Villa, R.; et al. Aficamten or Metoprolol Monotherapy for Obstructive Hypertrophic Cardiomyopathy. N. Engl. J. Med. 2025, DOI: 10.1056/NEJMoa2504654.
- FirstWord Pharma. As Cytokinetics awaits FDA approval decision, phase 3 cardio win sends stock soaring.
- Fierce Biotech. FDA delays decision date on Cytokinetics' heart drug to year-end in unusual safety program back-and-forth.
- Bristol Myers Squibb. Camzyos (mavacamten) Prescribing Information and REMS Program.
- Tenaya Therapeutics. MyPEAK-1 Trial (NCT05836259).
- Imbria Pharmaceuticals. IMPROVE-HCM Trial (NCT04826185).
- ESC Congress 2025. Safety, tolerability, pharmacokinetics and pharmacodynamics of HRS-1893 in patients with obstructive hypertrophic cardiomyopathy: a randomized, double-blind, placebo-controlled phase 1 trial. Presented Aug 2025.
Disclaimer: This article is for informational purposes only and does not constitute medical or investment advice. Readers should consult primary literature and official regulatory sources for verification.